
A Checklist for Opioid Prescribers
How is it possible that the opioid addiction epidemic is on the rise? This seems contradictory to the long- supported research in the article “Addiction Rare in Patients Treated with Narcotics”, published in the January 1980 New England Journal of Medicine. Pain coverage continues to be a highly debated topic and it’s not getting any easier for the prescribers. With the complication of patient satisfaction tied to provider reimbursement, this just adds to the difficulty for providers to objectively address chronic pain.
It’s worth noting that the NEJM study only involved hospitalized patients undergoing administration of small doses of opioids for acute pain during hospitalization, and therefore these patients were not given outpatient opioid prescriptions to continue after discharge. Results did show that only 4 cases out of 11,882 had a history of addiction and subsequently had documented inpatient opioid addiction after pain treatment (H. Jacobs, May 2016, Business Insider).
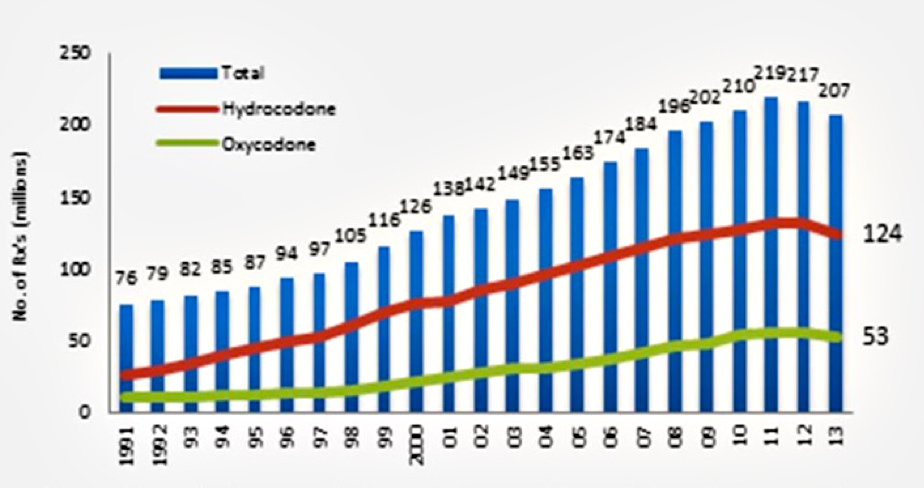
Source: National Institute on Drug Abuse
For almost two decades, opioid treatment for chronic pain not acute has been the real issue. The 2012 National Health Interview Survey reports a chronic pain prevalence for adults in the US as approximately 11.2%. As of 2011, the number of prescriptions written for narcotics has peaked, but unfortunately the overdose death rate continues to rise. According to the CDC, 78 Americans die every day from an opioid overdose and the number of opioid prescriptions and deaths from prescription opioids has quadrupled since 1999, but the reports on the amount of pain remain unchanged. The overdose death rate is a result of prescription opioid pain relievers and illicit opioids such as heroin. Sadly, the strongest risk factor for heroin usage is previous abuse of prescription opioids. The wide availability and low price of heroin continues to fuel the epidemic. From 2013 to 2014, the death rate from overdose of natural and semi-synthetic opioids (ex. morphine, oxycodone and hydrocodone) continued at a smooth upward trend increasing by 9% whereas a significant spike was evident for synthetic opioids (ex. fentanyl) overdose deaths doubling in one year and heroin overdose deaths increasing by 26%. States with the highest drug overdose rates include West Virginia, New Mexico, New Hampshire, Kentucky and Ohio.
Source: National Vital Statistics System, Mortality file
To help providers determine the best approach to chronic pain treatment, the CDC has compiled a checklist for prescribing opioids to adults over 18 for chronic pain longer than 3 months duration excluding cancer, palliative and end of life care.
This checklist includes:
1) when to initiate or continue opioids for chronic pain
2) opioid selection, dosage, duration, F/U, discontinuation
3) assessing risk and addressing harms of opioid use
The goal is to open a dialogue between the patient and provider regarding the risks and benefits of opioid therapy for chronic pain in order to ultimately improve the safety and effectiveness of pain treatment. If the provider is able to successfully convey the significant risks associated with chronic opioid use, the patient may be more likely to try other options without adversely affecting patient satisfaction.





