Avoid Denials and Mitigate Risk Under the CMS CERT Program
Insufficient documentation is by far the most common reason for denying a claim or improperly paying a claim. Improperly paid claims become problematic after identification by the Center for Medicare and Medicaid Services (CMS) Comprehensive Error Rate Testing (CERT), a random sampling of claims evaluated for compliance with Medicare coverage, coding and billing rules.
After a claim has been identified by CERT, an initial request for records and documentation is sent to the submitting provider or supplier via a medical record documentation request. Up to three subsequent requests for information are sent if no additional documentation is received after the initial request. To avoid being unnecessarily placed in the “No Documentation” error category, requests should be addressed and completed within 75 days of the initial request. Depending on the adequacy of the additional documentation submitted, the CERT program will notify the Medicare Administrative Contractor (MAC) which one of the following five major error categories the claim has been assigned:
- No Documentation
- Insufficient Documentation
- Medical Necessity
- Incorrect Coding
- Other (duplicate payment, non-covered service, ineligible beneficiary)
While there is an appeals process, it is best to be proactive and avoid this time-consuming option.
Source: CMS CERT
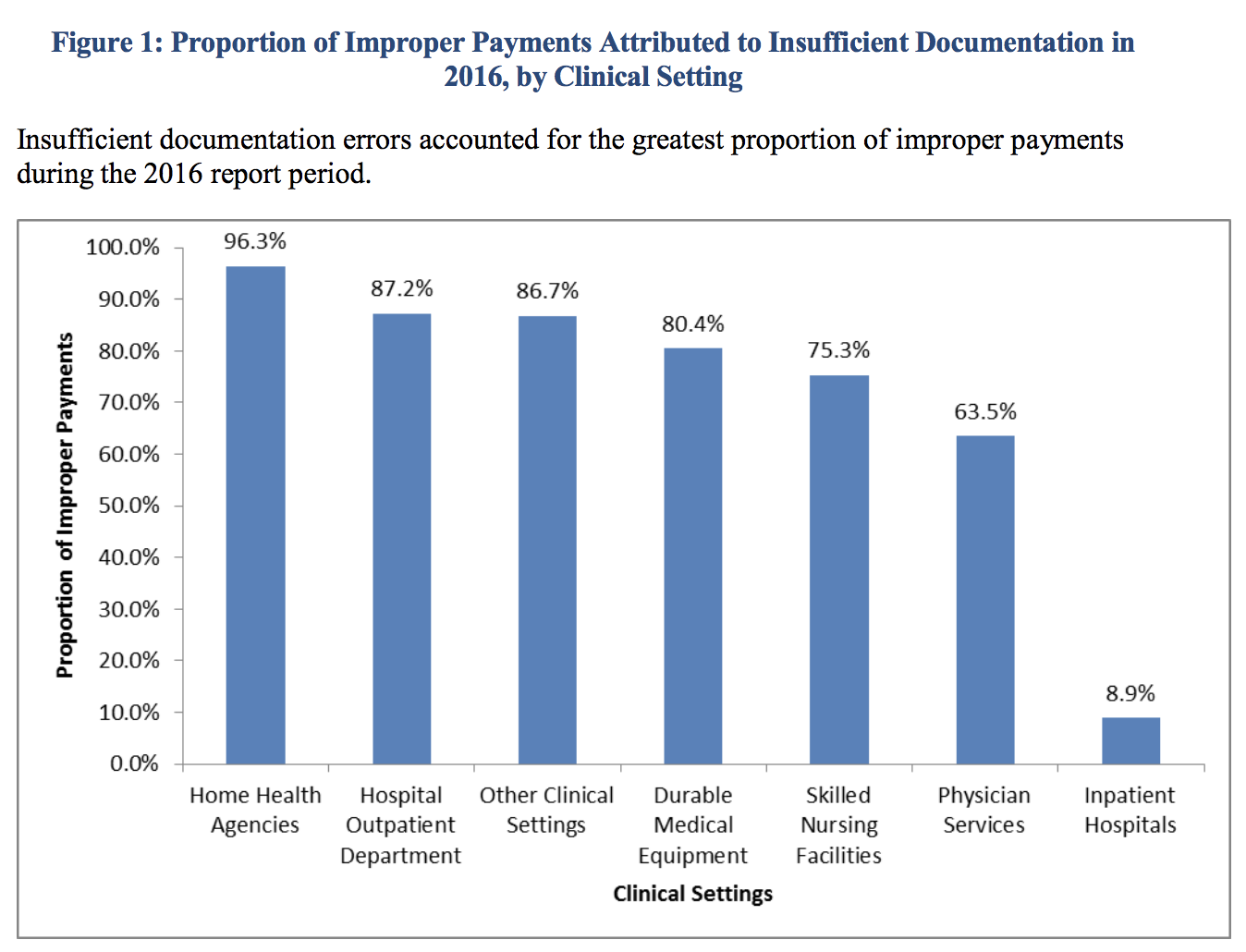
In all clinical settings, insufficient documentation accounts for the largest proportion of improper payments. Not meeting requirements for medical necessity is the second most common cause of improperly paid claims. In CMS’ Complying with Medical Documentation Requirements, CERT reviewers have identified common examples of insufficient documentation errors such as:
- Incomplete progress notes (unsigned, undated, insufficient detail)
- Unauthenticated medical records (no provider signature, no supervising signature, illegible signatures without a signature log or attestation to identify the signer, an electronic signature without the electronic record protocol or policy that documents the process for electronic signatures)
- No documentation of intent to order services and procedures (incomplete or missing signed order or progress note describing intent for services to be provided)
A few specific procedures and services are also under the watchful eye of CMS due to an association with a significant number of insufficient documentation errors and/or not meeting requirements for medical necessity. CMS offers resources for these outliers which include: Vertebral Augmentation Procedures (VAPs), Durable Medical Equipment (DME), Computed Tomography (CT) Scans, Evaluation and Management (E/M) and Physical Therapy (PT) services.
For FY2016 Medicare Fee-for-Service (FFS), the overall improper payment rate based on random sampling was 11.0%, a continued downward trend over the last two fiscal years. It’s also good news that the vast majority of claims are paid properly. The improper payment rate was highest with Durable Medical Equipment, Prosthetics, Orthotics and Supplies (46.26%) whereas Part A and B Providers had the highest estimated improper payment amounts, $22.01B and $10.93B respectively. MACs successfully recovered 86% of the total overpayment amount from FY2016.
According to CMS, CERT’s improper payment rates include overpayments and underpayments and should not be used interchangeably as a measure for fraud. Improperly paid claims are not necessarily fraudulent. However, any paid claim that is submitted fraudulently is always an improper payment. Subsequent identification of any unusual billing patterns and outlier claims will likely prompt further analysis by the CMS’ Fraud Prevention System.



